Data and Coordinating Center (DCC)
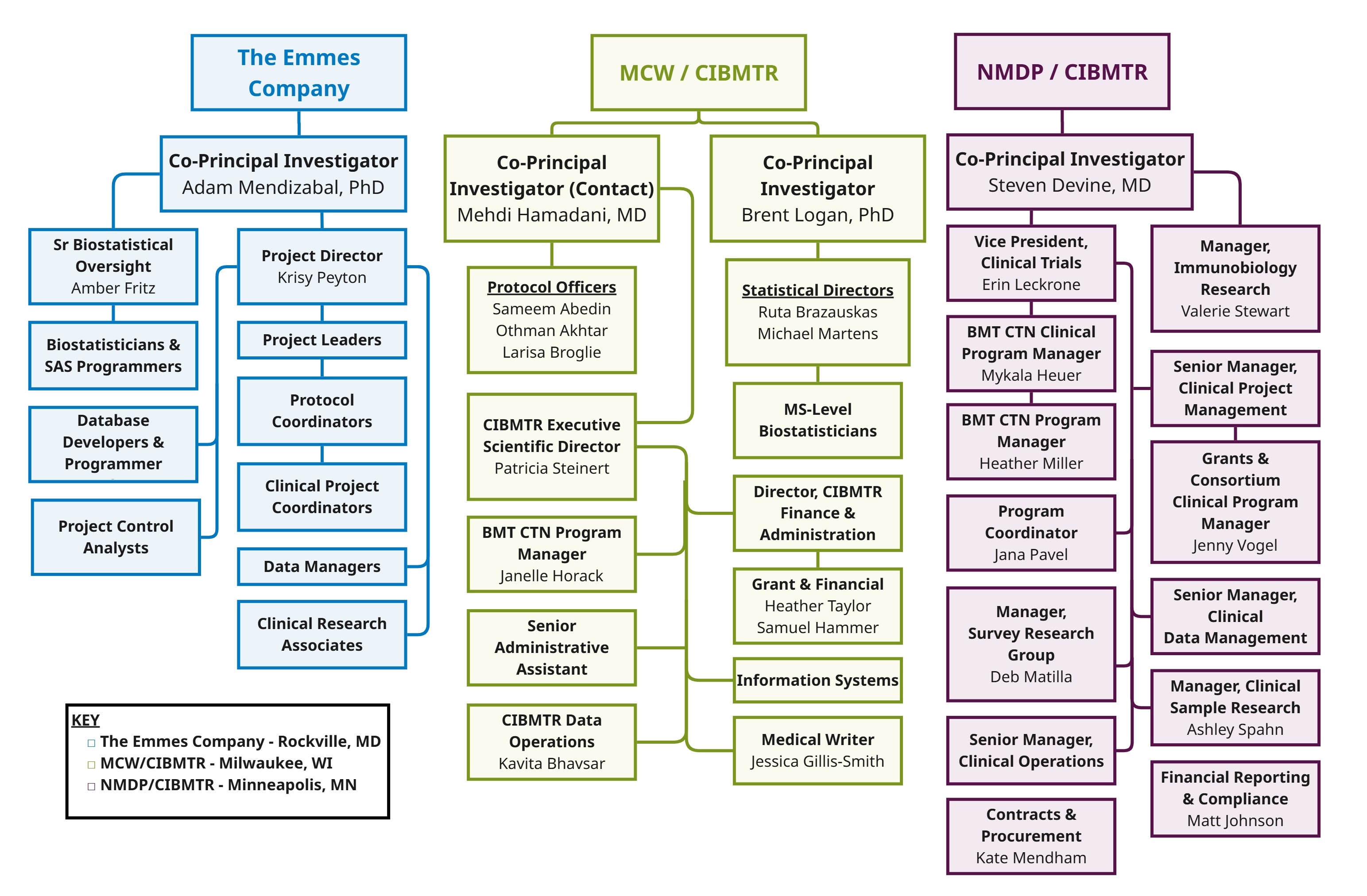
The BMT CTN Data and Coordinating Center (DCC) handles the overall coordination and administration of the BMT CTN program. Three organizations with extensive hematopoietic cell transplantation (HCT) and cellular therapy research experience manage the DCC.
The DCC is a collaboration of:
- Medical College of Wisconsin (MCW)*
- NMDP*
- The EMMES Company (EMMES)
* MCW and NMDP collaboratively operate the Center for International Blood and Marrow Transplant Research (CIBMTR).
The DCC supports and manages the efficient development, implementation, and completion of high-quality Phase II and III clinical trials for the Network by:
- Evaluating study concepts
- Developing protocols with appropriate statistical designs that are operationally feasible
- Facilitating review by independent experts, including a Protocol Review Committee, Data Safety and Monitoring Board, single Institutional Review Board and, where necessary, the Food and Drug Administration and other regulatory bodies
- Activating studies and developing plans to accrue in a timely manner
- Monitoring for safety and for regulatory and protocol compliance
- Collecting complete and accurate clinical, laboratory, and patient-reported outcomes data
- Analyzing and sharing research results
Core Clinical Centers
Nineteen institutions were awarded grants (cooperative agreements) by the National Heart, Lung, and Blood Institute and the National Cancer Institute to participate as Core Clinical Centers in the BMT CTN. Several of these grants were awarded to consortia of two or more centers. Core Center Principal Investigators, along with the NHLBI Program Officer, NCI Program Officer and the three DCC PIs have voting membership on the BMT CTN Steering Committee. The Steering Committee is responsible for the operation of the Network. The Steering Committee formulates and implements all policy decisions related to the work of the BMT CTN and establishes its scientific agenda.
The BMT CTN Core Clinical Centers bring the highest level of commitment and participation to the Network and facilitate collaboration among researchers, transplant center staff, and support personnel. The Network offers opportunities for patients across the US to access trials, and it provides a forum for shared ideas and resources for research. The heterogeneity of the community improves study validity. New approaches are tested in the broad range of centers in which they are ultimately applied.
Core Clinical Center staff carry out the provisions of the Manuals of Procedures and BMT CTN protocols and recruit, evaluate, and treat study participants. They are responsible for collecting all clinical, laboratory, demographic, and other data required by each BMT CTN study, including long-term follow-up. The Principal Investigator for each Core Clinical Center is directly responsible for ensuring that all aspects of BMT CTN protocols are followed. Other key center staff include other physicians, Co-Investigators, Clinical Research Associates/Coordinators, pharmacists, and related staff.
A list of Core Clinical Centers and Principal Investigators for the current project period, July 2024 through June 2031, may be seen here. As noted above Several Core Clinical Centers are Consortia of 2 or more centers.
Affiliate Centers
Participation in Network trials may be open to qualified centers other than Core Clinical Centers. These centers are referred to as “Affiliate Clinical Centers.” The DCC actively recruits appropriate Affiliate Clinical Centers for Network protocols within the limits of financial resources and in accordance with accrual needs of each protocol. Affiliate Clinical Centers are subject to the same quality assurance procedures as Core Clinical Centers.
Individuals with relevant expertise from Affiliate Clinical Centers may be nominated to participate in BMT CTN Technical Committees and Protocol Teams. Terms are the same as for individuals from Core Clinical Centers. Technical Committees and Protocol Teams are encouraged to have at least one Affiliate Clinical Center representative.
Affiliate Centers may earn voting representation on the Steering Committee for a renewable term of 2 years by exemplary performance in advancing the mission of the BMT CTN. At a minimum, this requires enrolling at least 12 patients on at least 2 Network trials during the previous year.
Steering Committee
The BMT CTN Steering Committee sets the Network’s scientific agenda and oversees the selection, design, execution, and analysis of all BMT CTN studies. Steering Committee members include leaders from a broad range of US transplant centers, which together conduct 77% of allogeneic hematopoietic cell transplantations in the country. The Committee meets monthly, three times a year in person (when possible), and otherwise by videoconference.
The Steering Committee consists of:
- Principal Investigators from Core Clinical Centers
- Representatives of high-performing Affiliate Centers selected by the Steering Committee
- NHLBI and NCI Project Officers
- DCC Principal Investigators (MCW, NMDP, Emmes)
- Representatives from the cooperative groups of the National Clinical Trials Network: ECOG-ACRIN, SWOG, Alliance for Clinical Trials in Oncology, and Children’s Oncology Group
The Steering Committee elects a Vice-Chair to a one-year term, followed by one-year term as Chair-elect, a two-year term as Chair and a one-year term as Immediate Past-Chair. At any given time, therefore, the Steering Committee Officers comprise a Chair, a Vice-Chair and either a Chair-elect or Immediate-Past Chair, all of whom must be Principal Investigators of Core Clinical Centers.
Executive Committee
The Executive Committee comprises the Steering Committee Chair, Vice-Chair, Chair-elect or Immediate Past-Chair, National Heart, Lung, and Blood Institute and National Cancer Institute Project Officers, and the DCC Principal Investigators. The Committee develops Steering Committee agendas and recommendations for the Steering Committee’s consideration. The Executive Committee provides direction between meetings of the Steering Committee and reviews/approves all non-protocol-specified ancillary studies and secondary analyses. The Executive Committee also provides an initial review of proposals for trials submitted for consideration by the BMT CTN to determine suitability for the Network. The Executive Committee meets monthly by video teleconference.
Protocol Teams
A Protocol Team is appointed for each approved Study Concept. The Protocol Team has primary responsibility for developing all protocol documents and meets weekly-monthly by teleconference throughout the lifecycle of the study.
The Protocol Team consists of:
- Protocol Chair(s)
- Core and Affiliate Clinical Center Investigators (3 or more)
- Protocol Officer (DCC physician)
- Primary Protocol Statistician (DCC statistician)
- Protocol Coordinator (DCC Coordinator)
- National Heart, Lung and Blood Institute (NHLBI) and National Cancer Institute representatives (1 each)
- NHLBI Statistician (1)
- DCC Business Representative
- Ad hoc members as deemed necessary by the Protocol Chair(s) and DCC
Technical Committees
Ad hoc Technical Committees conduct specified functions of Network activity, advise the Steering Committee on Network policies and procedures, and provide technical expertise for protocol design. Each Technical Committee has a DCC representative responsible for coordinating Committee conference calls and meetings. Each also has a representative from the National Heart Lung and Blood Institute (NHLBI) and the National Cancer Institute (NCI). The DCC representative works with the Committee Chair to prepare and distribute an agenda and minutes for each meeting and to ensure that the Committee’s findings are communicated to protocol teams, where appropriate (see below). The Network solicits nominations for Technical Committee members annually from participating Core and Affiliate Clinical Centers. Committee members consist of a maximum of ten members who are not associated with the DCC, NHLBI or NCI and are appointed by the Nominating or Executive Committee to three-year terms. The Steering Committees approve candidates to fulfill the 3-year term.
The following Technical Committees must review all BMT CTN protocols at some point in their development but no later than time of submission to the Protocol Review Committee: Biomarkers, Clinical Research Associates, Pharmacy, Special Populations, and Toxicity and Supportive Care.
Biomarkers Committee
The Biomarkers Committee comprises Core and Affiliate Center transplant physicians and seeks to:
- Inform the Network’s scientific agenda focusing on questions involving analysis of biologic specimens for genomic and proteomic markers
- Establish principles for specimen collection (including their use in Ancillary Studies)
- Review new and existing studies for opportunities to collect blood and tissue samples for analysis of potential prognostic markers
- Advise the Network protocol teams in their review of ancillary study proposals that request the use of BMT CTN-related research samples
For a current roster please see here.
Clinical Research Associates (CRA) Committee
The Clinical Research Associate Committee consists of CRAs and Data Managers from Core and Affiliate Centers and seeks to:
- Review each BMT CTN protocol before distribution to centers, focusing on reviewing and resolving supply chain issues and logistical issues (e.g., shipping and receipt of specimens or drugs, enrollment procedures, schedule of assessments, required observations)
- Assist in developing and reviewing Case Report Forms and data collection systems for specific protocols
- Consider solutions for logistical issues identified after study activation
- Review educational materials for research staff at participating clinical centers
- Provide input for the BMT CTN Coordinators’ meeting held during the BMT Tandem Meetings of American Society for Transplantation and Cellular Therapy (ASTCT) & Center for International Blood and Marrow Transplant Research (CIBMTR)
For a current roster please see here.
Dissemination and Implementation Committee
The Dissemination and Implementation Committee consists of Core and Affiliate Center transplant physicians and seeks to:
- Educate BMT CTN stakeholders in aspects of dissemination and implementation.
- Participate in protocol development and review to identify opportunities to embed implementation outcomes in the study design, identify stakeholders required for wide dissemination, and develop active dissemination approaches targeting specific stakeholders.
- Proactively identify potential challenges to and assessment of implementation based on “what-if” scenarios.
- Support dissemination and implementation strategies following study completion across all transplant programs, with particular emphasis on addressing inequities in implementation.
- Assess how implementation of protocol findings could address healthcare inequities by evaluating their impact on different populations.
- Define metrics for evaluation of dissemination and implementation strategies for incorporation into protocol designs.
For a current roster please see here.
Patient and Caregiver Advocacy Committee
The Patient and Caregiver Advocacy Committee (PCAC) consists of members involved with transplant either as a patient, caregiver, family member, donor, healthcare provider, or staff person/volunteer with an agency that interacts with HCT patients or donors. This committee seeks to:
- Identify areas of research most important to patients and caregivers.
- Advise the BMT CTN on ways to increase patient participation in research with a focus on increasing access to a diverse group of patients.
- Provide feedback on patient and caregiver-facing materials such as informed consents, website and social media content, study updates, and results summaries.
- Promote awareness among patients regarding research opportunities.
- Address misconceptions about clinical trial participation.
For a current roster please see here.
Pharmacy Committee
The Pharmacy Committee consists of transplant physicians and pharmacists from Core and Affiliate Centers and seeks to:
- Review all BMT CTN protocols for use, dosing, administration, and potential interactions of pharmaceuticals
- Develop a pharmacopoeia for commonly used drugs on BMT CTN protocols
- Advise Protocol Teams on possible ancillary studies, e.g. pharmacokinetic
For a current roster please see here.
Publication/Presentation Committee
The Publication/Presentation Committee is responsible for developing publication and presentation policies. All policies must be approved by the Steering Committee before implementation. The Committee reviews all proposed publications and presentations to ensure the protection of proprietary information and study participant confidentiality and to determine the public impact of publication and/or presentation of incomplete or premature results.
The Committee also provides input on authorship issues and appropriate grant acknowledgement. No individual institution or collaborator may present or publish individual findings from work performed on or data resulting from study protocols without the approval of the Publications Committee, NHLBI, and NCI.
For any questions, please contact bmtctnpublications@nmdp.org
Scientific Advisory Committee
There are twelve Scientific Advisory Committees. Each consists of Core and Affiliate Center transplant physicians with expertise in the committee topic.
Special Populations (Pediatrics / Human Subjects) Committee
The Special Populations Committee consists of pediatric and adult transplant physicians from Core and Affiliate Centers as well as an ethicist and seeks to:
- Ensure that children, women, and individuals from under-represented minority groups (URGs) are considered for inclusion in all protocols developed by the BMT CTN, with an appropriate plan to ensure access
- Evaluate all protocols before distribution to centers for potential barriers to enrollment by children, women, and individuals from URGs
- Ensure that, for studies involving pediatric participants, differences in obtaining informed consent/assent, patient care, and monitoring are appropriately addressed
- Recommend policies to increase diversity of patients accrued to BMT CTN trials
For a current roster please see here.
Toxicity and Supportive Care Committee
The Toxicity and Supportive Care Committee consists of Core and Affiliate Center transplant physicians and seeks to:
- Work with the DCC to define methods for evaluating adverse events and toxicities after hematopoietic cell transplantation and cellular therapy
- Review the evaluation and monitoring requirements for toxicities on BMT CTN protocols
- Review routine supportive care practices which are being considered during protocol development to avoid requiring unnecessary protocol-specific supportive therapies that may limit patient accrual
- Design and approve forms and procedures for collecting toxicity data, including standards for expedited reporting of certain adverse events
- Review each protocol before release to centers for appropriateness of toxicity assessments and supportive care therapies
For a current roster please see here.
Ad Hoc Committees
Additional administrative and technical committees are convened as needed to discuss new study concepts, provide an update to the Steering Committee on recent advances in the field, or provide input into the Network’s Technical Procedures. These have included committees addressing issues in Graft-versus-Host Disease, Nonmalignant Blood Diseases, Graft Characterization, Cellular Therapy, Late Effects/Quality of Life, and Myeloma and Infectious Disease.
Protocol Review Committee
The Protocol Review Committee (PRC) is an independent body appointed by the National Heart, Lung, and Blood Institute (NHLBI). The PRC performs the first step in the review process for BMT CTN protocols, evaluating the protocol for its scientific merit. The PRC may either recommend approval of the protocol to NHLBI, or request that changes and/or clarifications are made.
The PRC assesses the scientific merit of each protocol using the following criteria:
- Importance of the question to be addressed
- Need for a multi-center network to meet objectives
- The merit of the experimental design, including appropriate controls
- Availability of adequate resources
- Adequacy and safety of study participant population and number of study participants,
- including appropriate representation of minorities, women, and children (if applicable)
- Appropriate recruitment strategies
- Adequacy of proposed plans for data acquisition, transfer, management, and analysis
- Adequacy of quality control of data collection and monitoring and overall coordination of protocol management
- Appropriateness of the plans to train center personnel to accomplish proposed research goals
The PRC includes a Chairperson and members whose experience reflects areas of expertise necessary to evaluate the scientific merit and design of BMT CTN protocols. Members may be added on an ad hoc basis to the Committee if expertise in a specific scientific area is needed.
Single Institutional Review Board of Record (sIRB)
Beginning July 1, 2017, the BMT CTN has utilized the NMDP Institutional Review Board (NMDP IRB) as the Network’s single IRB (sIRB). The sIRB provides ethical review and oversees patient safety while reducing the inefficiencies and burden of each clinical site conducting its own full IRB review. All BMT CTN Core and Affiliate Clinical Centers/Consortia must agree to participate in the sIRB. The only exception is for centers outside the US that must follow their country’s regulatory requirements for ethical board review.
The NMDP IRB is fully accredited by the Association for the Accreditation of Human Research Protection Programs. The members of the NMDP IRB are a diverse group of distinguished healthcare professionals, donor advocates, and patient advocates with expertise in blood and marrow transplantation and hematology/oncology.
The NMDP IRB meets monthly and conducts study-specific reviews as required by the regulations. This includes initial review, continuing review, and review of amendments/modifications to previously approved research. Additionally, any other study-specific documents submitted to the NMDP IRB are reviewed per the NMDP IRB Standard Operating Procedures and federal regulations. Administrative functions of the NMDP IRB are managed by NMDP Human Research Protection Program staff members.
Data and Safety Monitoring Boards
The Data and Safety Monitoring Boards (DSMB) are independent bodies appointed by the National Heart, Lung, and Blood Institute. There are currently two DSMBs, each having a separate list of studies for review.
Following approval by the Protocol Review Committee, the DSMB reviews protocols, focusing on monitoring plans, data quality and safety assurance. The DSMB may recommend approval and/or request changes. Each Board consists of a Chairperson and members with expertise in hematopoietic cell transplantation and cellular therapy, biostatistics, clinical trials, bioethics, and the specific research areas of Network studies.
After approving the protocol, the DSMB regularly monitors the data from the clinical trial, reviews and assesses the performance of its operations, and makes recommendations, as appropriate, to the National Institutes of Health concerning:
- Benefits/risks ratio of procedures and the burden under which the study participants are placed
- Completeness, quality, and analysis of measurements that are made
- Performance of individual centers (including possible recommendations on actions to be taken regarding any center that performs unsatisfactorily)
- Interim results of the study for evidence of efficacy or adverse effects
- Possible early termination of the study because of early attainment of study objectives, efficacy, and/or safety concerns, or, if applicable, inadequate performance or accrual
- The desirability of proceeding to the full-scale trial at the completion of the feasibility phase, when applicable
- Possible modifications/amendments to the study protocol and/or consent form(s)